Health on the Frontlines: COVID and Monkeypox, Where Are We Going?
Historically, coronaviruses become more contagious through mutation and less lethal so as not to kill their human host as often. It’s not the virus that kills directly. It’s our immune response of inflammation and clotting to the virus that causes the severe disease progression. Looking back at hundreds of thousands of medical charts, we now know that certain factors increase the risk of being hospitalized, ending up on a respirator or dying. It is now clear that 78% of the COVID deaths were in overweight elevated BMI individuals who were older.
Another fascinating finding was that those with high vitamin D levels of 50 and higher fared much better avoiding hospitalization and death as compared to those with low vitamin D levels. We also learned that the antioxidant glutathione was lower in those who did not do as well with COVID and were hospitalized. Another interesting finding was that diabetics had more problems, but diabetics on a drug used for diabetes made from the French lilac metformin did better with a lower death rate.
Unfortunately, the current vaccines and boosters are for the original alpha Wuhan variant, not for the current dominant Omicron or BA.2 subvariants. The vaccine still creates enough of an immune stimulus to shield against severe disease. Since February 2022, 40% of the deaths are in fully vaccinated persons and 60% of the deaths are in unvaccinated persons. Interestingly enough, people who are unvaccinated, had COVID and survived are testing positive less often.
Substantial consideration should be given to allowing healthcare workers who had it to return to work even if unvaccinated. This is why the CDC does not require a COVID test for patients who had and recovered from COVID within 90 days to enter the USA from abroad without a test. Variant-specific vaccines are on their way. The IV antibodies and new antivirals have made us all safer.
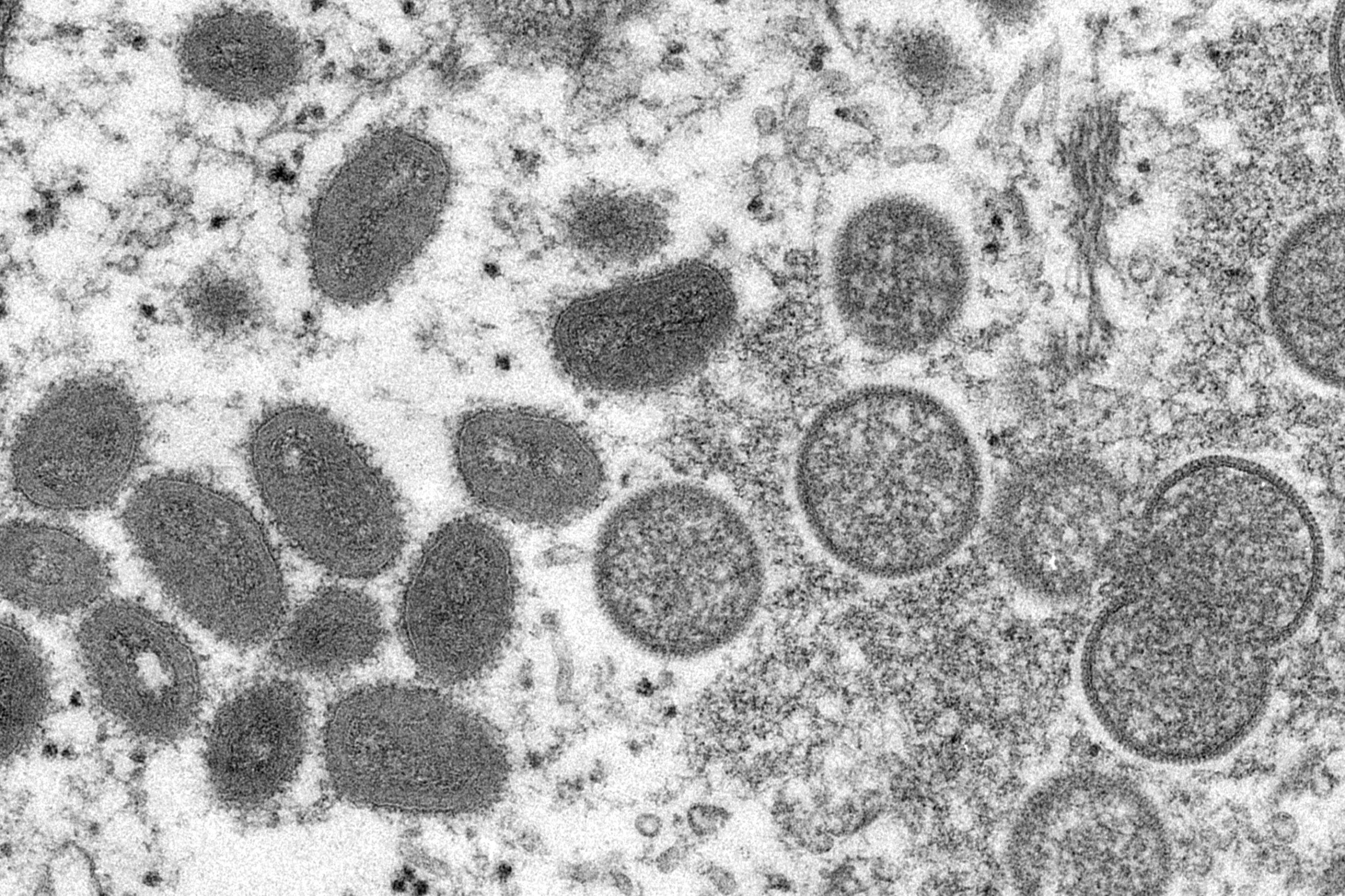
Next, we will keep an eye on the monkeypox virus that is now spreading around the world with cases confirmed in NYC and Massachusetts. It is a DNA virus unlike RNA coronaviruses. The difference is that it causes rashes and pustules of the skin and lymph nodes to be swollen.
The good news is a vaccine was approved in the USA for monkeypox in 2019 that is 85% effective and the current administration ordered millions of doses this year. The current administration did a very smart move by forming the pandemic innovation task force supported by one democratic senator from Washington state and a republican senator from North Carolina. This group with its bipartisan support will keep us safer and prepared. There is no good treatment for monkeypox virus at this time and it is fatal in 3–6% of cases.
It was first discovered in a colony of monkeys in Africa 50 years ago. The new concern is that the cases in Spain, the UK and Northern Portugal have been mostly new in gay and bisexual men. It is best to avoid contact when fever, chills, pustules are present. Scientists are searching for new antivirals as we speak to manage this outbreak. We now realize healthcare is national security. It’s great to see a unified approach to solving these health challenges that are confronting our generation.
Think positive and test negative. This too shall pass.
Peter Michalos, MD is associate professor of clinical ophthalmology, Columbia University VP&S; chairman, Hamptons Health Society; and a Southampton resident.
Vetted Hamptons Resources



